
How Much Vitamins Is Too Much? Understanding Supplement Upper Limits#
Taking vitamins and supplements has become a daily habit for millions of people worldwide. But more is not always better. Every vitamin has a threshold above which it stops being helpful and starts being harmful. This threshold is called the Tolerable Upper Intake Level (UL) — and understanding it is one of the most important things you can do for your supplement safety.
Vitamin toxicity is more common than most people realize. A 2023 study published in the American Journal of Clinical Nutrition found that approximately 30% of supplement users exceed the recommended upper intake level for at least one nutrient, often without knowing it. The consequences range from mild digestive discomfort to serious organ damage, depending on the substance and the degree of excess.
This comprehensive guide covers the supplement upper limits for every substance supported by 7iu.net, explains the difference between fat-soluble and water-soluble vitamin risks, and provides practical guidance for safe vitamin doses that protect your health.
What Is the Tolerable Upper Intake Level (UL)?#
The Tolerable Upper Intake Level (UL) is defined by the NIH Office of Dietary Supplements as:
"The highest level of daily nutrient intake that is likely to pose no risk of adverse health effects for almost all individuals in the general population."
The UL is established by the Food and Nutrition Board of the National Academies of Sciences, Engineering, and Medicine (formerly the Institute of Medicine). It is based on a systematic review of clinical evidence, animal studies, and case reports of adverse effects.
Key points about the UL:
- It is not a recommended dose. The UL is a safety ceiling, not a target. Most people need far less than the UL for optimal health.
- It applies to total daily intake from all sources — food, fortified foods, beverages, and supplements combined.
- Exceeding the UL does not guarantee harm, but it significantly increases the probability of adverse effects. The risk generally increases with the magnitude and duration of excess intake.
- The UL varies by age group. Children, adolescents, and adults have different thresholds. The values in this guide refer to adults unless otherwise stated.
The World Health Organization (WHO) and regulatory bodies such as the European Food Safety Authority (EFSA) publish similar upper intake guidelines, though exact numbers may vary slightly between jurisdictions.
Why Knowing the UL Matters: Fat-Soluble Vitamin Accumulation#
Not all vitamins carry the same risk of toxicity. The critical distinction is between fat-soluble and water-soluble vitamins, and this difference is the primary reason why understanding the tolerable upper intake level is so important.
Fat-soluble vitamins (A, D, E, K) dissolve in fat and are stored in your liver and adipose (fatty) tissue. Because your body cannot easily excrete excess amounts, these vitamins accumulate over time. Chronic overconsumption can lead to toxic levels building up in your body over weeks or months, even if each individual dose seems modest. This accumulation effect is why fat-soluble vitamins have clearly defined ULs and why vitamin overdose with these substances is a genuine medical concern.
Water-soluble vitamins (C, B-complex) dissolve in water and are generally excreted through urine when consumed in excess. While water-soluble vitamin toxicity is less common, it is not impossible — extremely high doses of Vitamin B6, for example, can cause nerve damage. However, the safety margin is typically much wider than for fat-soluble vitamins.
The bottom line: fat-soluble vitamins require more caution, more careful dose tracking, and more awareness of cumulative intake from multiple sources.
Fat-Soluble vs Water-Soluble Vitamins: Toxicity Risk Comparison#
| Characteristic | Fat-Soluble (A, D, E, K) | Water-Soluble (C, B-complex) |
|---|---|---|
| Storage in body | Stored in liver and fat tissue | Minimal storage; excreted in urine |
| Accumulation risk | High — builds up over time | Low — excess is generally eliminated |
| Toxicity onset | Gradual (weeks to months) | Usually requires very high acute doses |
| UL defined? | Yes, for most | Yes for some; wider safety margins |
| Primary concern | Chronic overconsumption from supplements | Mega-dosing; less common at typical doses |
| Reversibility | Often reversible if caught early | Usually quickly reversible |
Complete Supplement Upper Limits Table#
The following table covers all substances supported by 7iu.net, with UL values sourced from the NIH Office of Dietary Supplements and the National Academies Dietary Reference Intakes (DRI) reports.
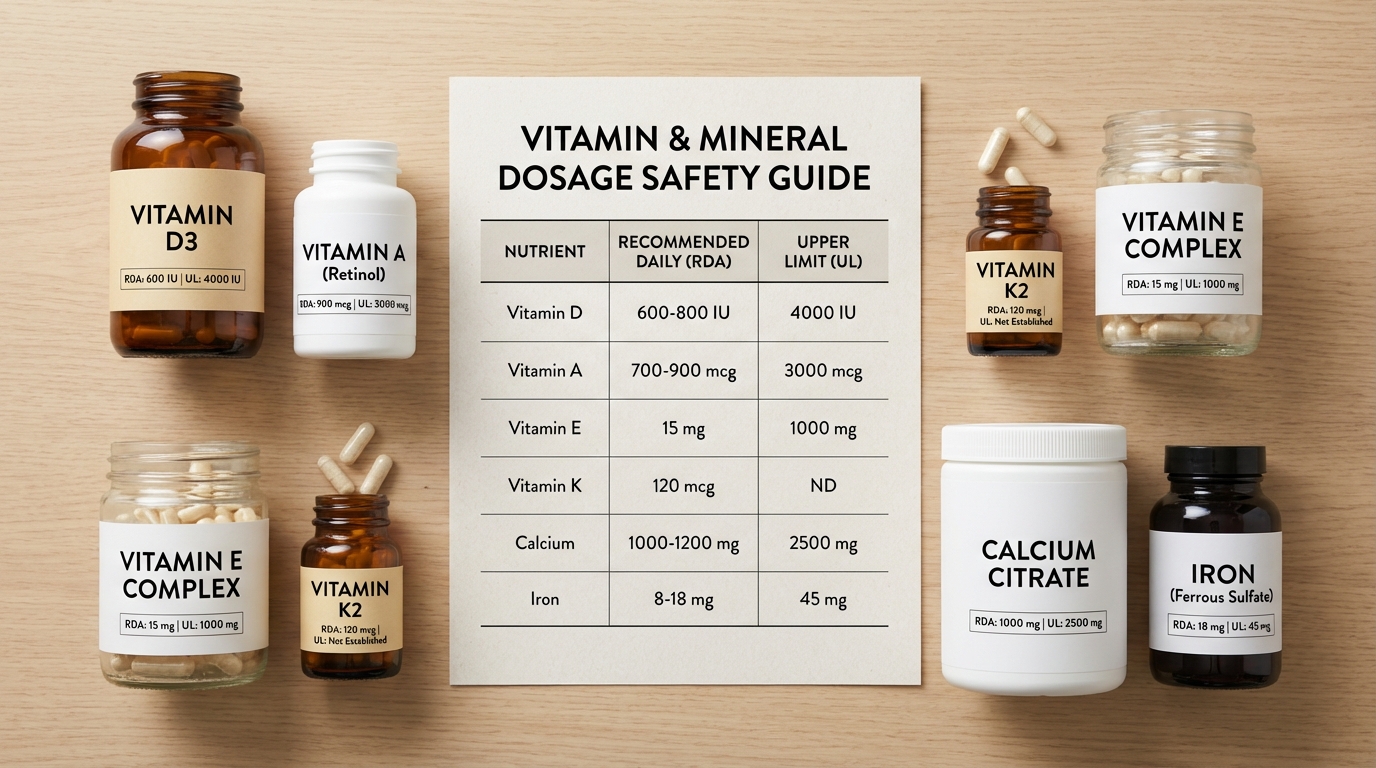
| Substance | UL (IU/day) | UL (Metric/day) | Solubility | Risk Level |
|---|---|---|---|---|
| Vitamin D3 (cholecalciferol) | 4,000 IU | 100 mcg | Fat-soluble | Moderate |
| Vitamin A — Retinol (preformed) | 10,000 IU | 3,000 mcg RAE | Fat-soluble | High |
| Vitamin A — Beta-Carotene | No established UL* | No established UL* | Fat-soluble | Low (from food) |
| Vitamin E — Natural (d-alpha-tocopherol) | 1,493 IU | 1,000 mg | Fat-soluble | Moderate |
| Vitamin E — Synthetic (dl-alpha-tocopherol) | 2,222 IU | 1,000 mg | Fat-soluble | Moderate |
| Insulin (human) | N/A — prescription drug | N/A | N/A | Rx only |
*Beta-carotene from food has no established UL because the body self-regulates its conversion to Vitamin A. However, high-dose beta-carotene supplements (20-30 mg/day) have been associated with increased lung cancer risk in smokers and former smokers, based on findings from the ATBC and CARET clinical trials published in the New England Journal of Medicine and cited by the NIH.
Insulin is a prescription medication, not a dietary supplement. It does not have a UL in the nutritional sense. Insulin dosing is determined individually by a healthcare provider based on blood glucose levels, body weight, and other clinical factors. For information about insulin dosing, see our insulin unit conversion guide.
Overdose Symptoms by Substance#
Understanding the warning signs of vitamin overdose can help you identify a problem before it becomes serious.
Vitamin D3 Toxicity (Hypervitaminosis D)#
Excess Vitamin D causes the body to absorb too much calcium, a condition called hypercalcemia. Symptoms include:
- Nausea, vomiting, and poor appetite
- Excessive thirst and frequent urination
- Weakness and fatigue
- Kidney stones and potential kidney damage
- Confusion and disorientation
- Heart rhythm abnormalities in severe cases
Toxicity typically occurs at sustained daily intakes above 10,000 IU and blood levels of 25(OH)D exceeding 150 ng/mL. For a detailed discussion, see our Vitamin D toxicity and upper limit guide.
Vitamin A (Retinol) Toxicity (Hypervitaminosis A)#
Preformed Vitamin A is the most dangerous of the common supplements when taken in excess. Symptoms of acute toxicity (single very large dose) include:
- Severe headache and blurred vision
- Nausea, vomiting, and dizziness
- Skin peeling
Chronic toxicity (prolonged overconsumption above the UL) can cause:
- Liver damage (hepatotoxicity) — the most serious long-term consequence
- Bone thinning and increased fracture risk
- Hair loss and dry, cracking skin
- Birth defects if taken during pregnancy (retinol is a known teratogen)
The NIH reports that liver damage can occur with chronic intake of just 25,000 IU/day in adults. For more information, see our Vitamin A toxicity guide.
Vitamin E Toxicity#
Vitamin E toxicity is less common than Vitamin A or D toxicity, but it carries a unique risk. High-dose Vitamin E supplements (above the UL of 1,000 mg/day) can:
- Increase the risk of hemorrhagic stroke — Vitamin E has anticoagulant properties that interfere with blood clotting
- Cause nausea, diarrhea, and abdominal cramps
- Interact dangerously with blood-thinning medications (warfarin, aspirin)
- Potentially increase all-cause mortality at doses above 400 IU/day, based on a meta-analysis published in the Annals of Internal Medicine
The anticoagulant effect is particularly concerning for patients about to undergo surgery or those already on antiplatelet therapy.
Insulin Overdose#
Although insulin is not a supplement, it is relevant to mention here because 7iu.net provides insulin conversion tools. An insulin overdose causes hypoglycemia (dangerously low blood sugar), which can result in:
- Trembling, sweating, and rapid heartbeat
- Confusion and difficulty speaking
- Seizures
- Loss of consciousness
- Death in severe untreated cases
Insulin overdose is a medical emergency. If you suspect an insulin overdose, call emergency services immediately.
The Hidden Risk: Supplement Stacking#
One of the most overlooked causes of exceeding safe vitamin doses is supplement stacking — taking a multivitamin alongside standalone supplements that contain the same nutrients.
Consider this common scenario: You take a daily multivitamin that contains 2,000 IU of Vitamin D3, plus a standalone Vitamin D3 supplement of 5,000 IU, plus a calcium-with-Vitamin-D tablet that contains 1,000 IU. Your total daily Vitamin D3 intake is 8,000 IU — double the UL of 4,000 IU — and you may not even realize it.
This problem is especially prevalent with:
- Vitamin A — found in multivitamins, prenatal vitamins, cod liver oil, and standalone supplements. The combined intake can easily exceed 10,000 IU.
- Vitamin D — added to multivitamins, calcium supplements, bone health formulas, and immune support products.
- Vitamin E — present in multivitamins, skin health supplements, and antioxidant blends.
How to avoid supplement stacking risks:
- List every supplement you take — including multivitamins, fortified foods, and specialty blends.
- Add up the total daily intake for each nutrient across all sources.
- Compare the total to the UL using the table above.
- Eliminate redundant supplements — if your multivitamin already provides adequate amounts, you may not need a standalone supplement.
How to Supplement Safely#
Following these evidence-based practices will help you stay within safe vitamin doses and avoid toxicity:
1. Audit All Your Sources#
Before adding any new supplement, inventory every source of that nutrient in your current regimen — including fortified foods (cereals, milk, orange juice), existing supplements, and prescription medications. Use our conversion tools to standardize units for easy comparison.
2. Get Blood Work Done#
For fat-soluble vitamins, especially Vitamin D and Vitamin A, periodic blood tests are the gold standard for monitoring status. Ask your doctor to check:
- 25(OH)D for Vitamin D status
- Retinol or retinyl esters for Vitamin A status
- Serum calcium to screen for hypercalcemia
Blood tests remove the guesswork and give you objective data to guide supplementation decisions.
3. Start Low, Increase Gradually#
If blood work indicates a deficiency, start with a moderate dose and retest after 2-3 months. Jumping to the maximum dose without monitoring is unnecessary for most people and increases the risk of overcorrection.
4. Consult Your Healthcare Provider#
This is especially important if you:
- Take prescription medications that may interact with supplements
- Have liver or kidney disease (impaired nutrient metabolism)
- Are pregnant or breastfeeding
- Take multiple supplements
- Plan to exceed the RDA for any nutrient
5. Choose Reputable Brands#
Look for supplements tested by independent laboratories such as USP (United States Pharmacopeia), NSF International, or ConsumerLab. Third-party testing verifies that the product contains what the label claims and is free from harmful contaminants.
Special Populations: Who Needs Extra Caution#
Certain groups face elevated risks from supplement overconsumption and may have different UL thresholds.
Pregnant and Breastfeeding Women#
- Vitamin A (retinol) is a known teratogen. Excess retinol during pregnancy is associated with birth defects affecting the heart, brain, and face. Pregnant women should not exceed 3,000 mcg RAE (10,000 IU) per day from preformed Vitamin A and should choose prenatal vitamins containing beta-carotene instead of retinol where possible.
- Vitamin D requirements may increase during pregnancy, but the UL remains 4,000 IU/day unless a physician prescribes otherwise based on blood work.
Children#
Children have lower ULs for all nutrients due to their smaller body mass. For example, the Vitamin D UL for children ages 1-3 is only 2,500 IU/day — well below the adult UL of 4,000 IU. Adult-dose supplements should never be given to children without medical guidance.
Individuals with Liver Disease#
The liver is the primary storage and processing organ for fat-soluble vitamins. People with liver disease (hepatitis, cirrhosis, fatty liver disease) may accumulate these vitamins more readily and experience toxicity at lower intake levels. Vitamin A is particularly hepatotoxic in this population — the NIH notes that people with liver disease can develop toxicity at intakes below the standard UL.
Individuals with Kidney Disease#
The kidneys play a central role in Vitamin D metabolism (converting 25(OH)D to the active form, 1,25(OH)2D). Patients with chronic kidney disease (CKD) require specialized forms of Vitamin D (such as calcitriol) and should only supplement under strict nephrology supervision. Standard Vitamin D3 supplementation in CKD patients carries unique risks of hypercalcemia and vascular calcification.
Convert Your Supplement Doses#
Not sure whether your supplement dose is within the safe range? Use our interactive calculator to convert between IU and metric units for quick comparison against the UL values listed above:
Quick Links: Substance-Specific Converters#
Use these dedicated converters to check exact values for each substance:
- Vitamin D3 IU to mcg converter — Convert your Vitamin D3 dose and compare to the 4,000 IU (100 mcg) UL
- Vitamin A (Retinol) IU to mcg converter — Check retinol doses against the 10,000 IU (3,000 mcg RAE) UL
- Vitamin E (Natural) IU to mg converter — Verify natural Vitamin E doses against the 1,493 IU (1,000 mg) UL
- Insulin Units to mg converter — Convert insulin units (prescription medication, not subject to UL)
- What is IU? Complete guide to International Units — Understand the unit system behind all these conversions
Key Takeaways#
- The Tolerable Upper Intake Level (UL) is the maximum daily dose unlikely to cause harm — not a target to aim for.
- Fat-soluble vitamins (A, D, E) accumulate in the body and carry higher toxicity risk than water-soluble vitamins.
- Vitamin A (retinol) is the most dangerous common supplement when taken in excess, with liver damage as the primary concern.
- Vitamin D3 toxicity causes hypercalcemia, which can damage kidneys and other organs. The adult UL is 4,000 IU/day.
- Vitamin E in high doses can increase hemorrhagic stroke risk due to its anticoagulant properties.
- Supplement stacking — taking a multivitamin plus standalone supplements — is a common and underappreciated cause of exceeding the UL.
- Blood tests are the most reliable way to monitor your vitamin status and avoid both deficiency and excess.
- Special populations (pregnant women, children, and those with liver or kidney disease) may need lower thresholds and closer monitoring.
- Always consult a healthcare provider before starting high-dose supplementation or if you suspect you have exceeded the UL.
Sources#
- NIH Office of Dietary Supplements — Vitamin D Fact Sheet
- NIH Office of Dietary Supplements — Vitamin A Fact Sheet
- NIH Office of Dietary Supplements — Vitamin E Fact Sheet
- National Academies — Dietary Reference Intakes (DRI) Tables
- WHO — Micronutrient Deficiencies
- American Diabetes Association — Insulin Basics
- Institute for Safe Medication Practices — High-Alert Medications